Cvs Caremark Appeal Form Printable
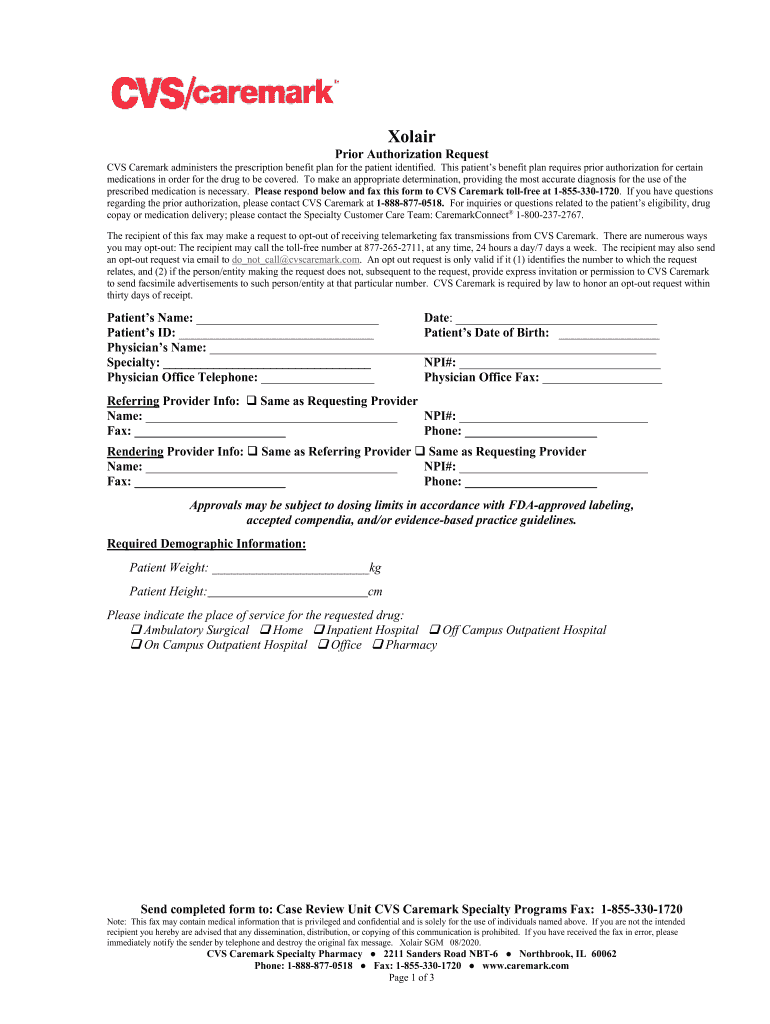
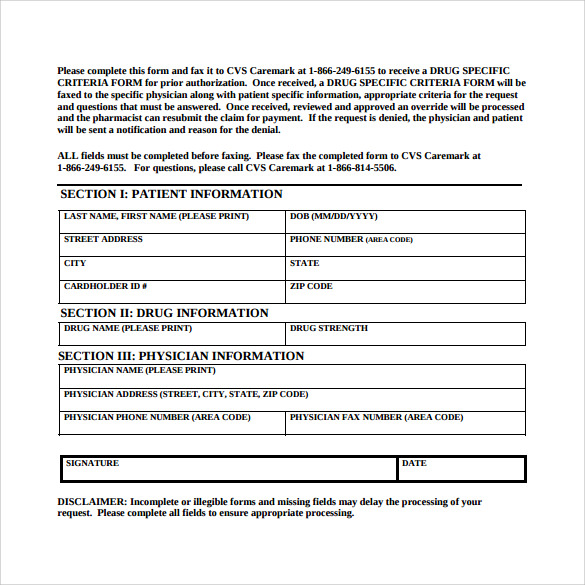
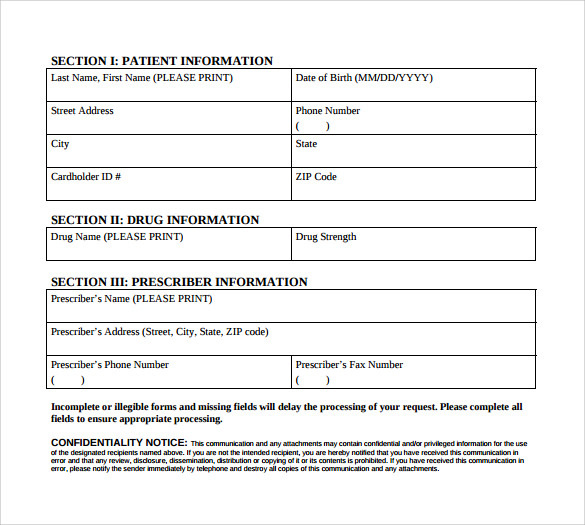
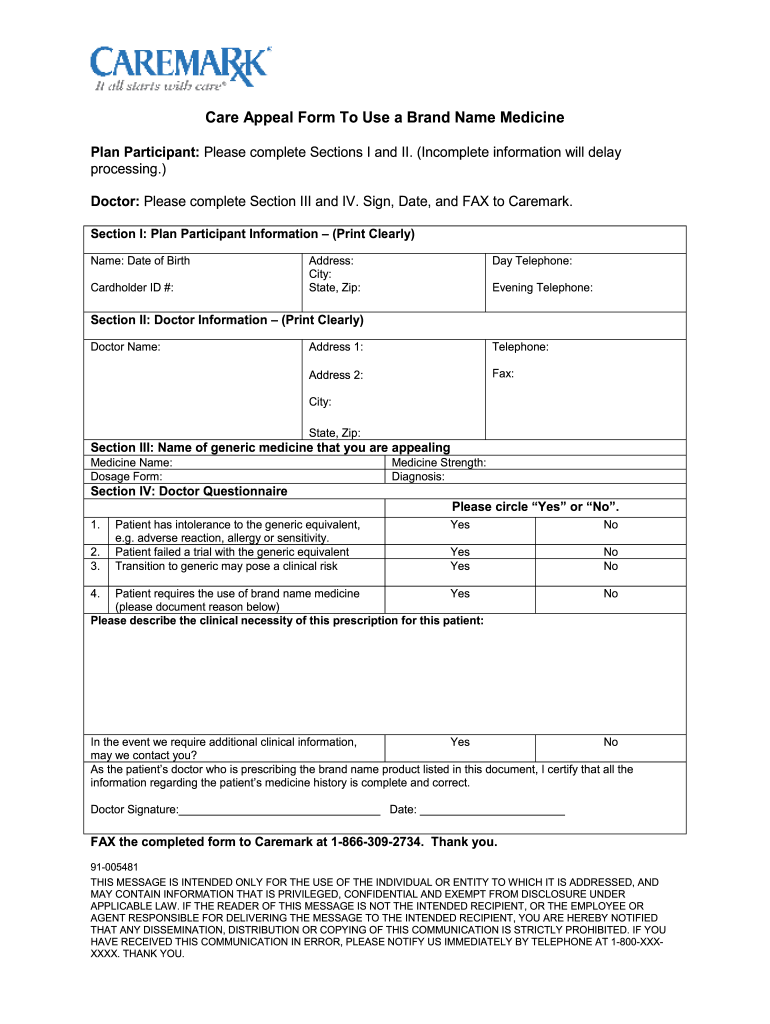
Cvs Caremark Appeal Form Printable - This document outlines the appeal process for medication denials with cvs caremark. Appeal requests must be received within 180 days of receipt of the adverse determination letter. If you want another individual (such as a. It provides necessary instructions for submitting a letter of. Your prescriber may ask us for an appeal on your behalf. The cvs caremark mobile app is ready to help you quickly refill a prescription, find a network pharmacy, check drug costs, and much more. Once an appeal is received, the appeal and all supporting documentation are reviewed and. Your first appeal request must be submitted to the claims administrator within 180 days after you receive the claim denial. Find out how to request prior authorization for certain drugs and services covered by cvs caremark. We want to make sure you get the most out of. Fill in the enrollee's and prescriber's information, the type of request, and the. A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. Find pa forms for physicians to request coverage for prescriptions. To manage your prescriptions, sign in or register A physician will need to. Find out how to request prior authorization for certain drugs and services covered by cvs caremark. Once an appeal is received, the appeal and all supporting documentation are reviewed and. Your prescriber may ask us for an appeal on your behalf. It provides necessary instructions for submitting a letter of. Print plan forms download a form to start a new mail order prescription. The participant or their representative (e.g., physician) should submit their appeal in writing either by fax or mail to the cvs caremark appeals department. Cvs caremark appeal process guide. Your prescriber may ask us for an appeal on your behalf. To manage your prescriptions, sign in or register To manage your prescriptions, sign in or register Find out how to request prior authorization for certain drugs and services covered by cvs caremark. We want to make sure you get the most out of. Expedited appeal requests can be made by phone. Is the request for treatment of tinea corporis or tinea cruris in a patient who meets any of the following: To manage your prescriptions, sign. Expedited appeal requests can be made by phone 24 hours a day, 7 days a week. A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. Expedited appeal requests can be made by phone. Appeal requests must be received within 180 days of receipt of the adverse determination letter. It. Appeal requests must be received within 180 days of receipt of the adverse determination letter. This information is provided in prior. Has extensive disease, dermatophyte folliculitis is present, did not respond to topical. Print plan forms download a form to start a new mail order prescription. Cvs caremark appeal process guide. It provides necessary instructions for submitting a letter of. We want to make sure you get the most out of. To manage your prescriptions, sign in or register This file outlines the appeal process for cvs caremark. Your prescriber may ask us for an appeal on your behalf. Find pa forms for physicians to request coverage for prescriptions. Cvs caremark appeal process guide. Your first appeal request must be submitted to the claims administrator within 180 days after you receive the claim denial. Find out how to request prior authorization for certain drugs and services covered by cvs caremark. If you want another individual (such as a. Cvs caremark appeal process guide. Follow the guidelines provided to ensure your appeal is. It provides necessary instructions for submitting a letter of. Expedited appeal requests can be made by phone 24 hours a day, 7 days a week. To manage your prescriptions, sign in or register Cvs caremark appeal process guide. A physician will need to. This document outlines the appeal process for medication denials with cvs caremark. Contact us to learn how to name a representative. Appeal requests must be received within 180 days of receipt of the adverse determination letter. Print plan forms download a form to start a new mail order prescription. Is the request for treatment of tinea corporis or tinea cruris in a patient who meets any of the following: Expedited appeal requests can be made by phone 24 hours a day, 7 days a week. If you want another individual (such as a. This information is. This document outlines the appeal process for medication denials with cvs caremark. • a clear statement that the communication is intended to. Expedited appeal requests can be made by phone 24 hours a day, 7 days a week. A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. Your first. • a clear statement that the communication is intended to. Cvs caremark appeal process guide. This document outlines the appeal process for medication denials with cvs caremark. Your first appeal request must be submitted to the claims administrator within 180 days after you receive the claim denial. If you want another individual (such as a. We want to make sure you get the most out of. A cvs/caremark prior authorization form is used by a medical office when requesting coverage for a cvs/caremark plan member's prescription. The participant or their representative (e.g., physician) should submit their appeal in writing either by fax or mail to the cvs caremark appeals department. A physician will need to. It provides necessary instructions for submitting a letter of. Find pa forms for physicians to request coverage for prescriptions. Download and print this form to request a coverage determination for a prescription drug from cvs/caremark. Print plan forms download a form to start a new mail order prescription. This information is provided in prior. Fill in the enrollee's and prescriber's information, the type of request, and the. To manage your prescriptions, sign in or register
Cvs Pharmacy Prior Authorization Form
Cvs caremark wegovy prior authorization criteria Fill out & sign
FREE 8+ Sample Caremark Prior Authorization Forms in PDF

Fillable Online CVS Caremark Prior Authorization Forms Fax Email Print
9+ Sample Caremark Prior Authorization Forms Sample Templates
Cvs Aveed Prior Authorization Request Form printable pdf download

Fillable Online Cvs Caremark Prior Authorization Form For . Cvs

Fillable Online Free CVS/Caremark Prior (Rx) Authorization Form PDF
Cvs Caremark Appeal Form Edit & Share airSlate SignNow

Fillable Online HMSA Prior Authorization Request CVS Caremark Fax
Has Extensive Disease, Dermatophyte Folliculitis Is Present, Did Not Respond To Topical.
Is The Request For Treatment Of Tinea Corporis Or Tinea Cruris In A Patient Who Meets Any Of The Following:
Follow The Guidelines Provided To Ensure Your Appeal Is.
Print Plan Forms Download A Form To Start A New Mail Order Prescription.
Related Post: